

AHM v. FDA reaches the Supreme Court
The plaintiffs' arguments are not so great.

Yesterday, the Supreme Court heard oral argument in FDA v. Alliance for Hippocratic Medicine. In this post, I will evaluate the strength of the plaintiffs’ contentions as expressed at the oral argument. Spoiler alert: there are some holes.
How we got here
If you already know about this case, you can skip to the next section. But for readers new to the case, the plaintiffs are groups of pro-life doctors and individual doctors who seek to ban or restrict the use of mifepristone, a drug used to terminate pregnancies.
The FDA approved mifepristone in 2000. In 2016, the FDA loosened certain restrictions on mifepristone’s use: it increased the gestational age limit from 49 to 70 days, reduced the number of required in-person clinic visits to one, and allowed healthcare providers other than doctors to prescribe the drug. In 2021, the FDA eliminated the in-person dispensing requirement.
The plaintiffs persuaded a federal district court to overturn all of the FDA’s orders. The district court’s decision—had it gone into effect—would have resulted in mifepristone being banned nationwide. On appeal, the Fifth Circuit reversed the district court’s decision insofar as it overturned the 2000 order, but upheld the district court’s decision insofar as it overturned the 2016 and 2021 orders.
In prior posts, I’ve expressed strong disagreement with both the district court’s decision and the Fifth Circuit’s decision. As I see it, the plaintiffs should have gotten no relief. There are two basic problems with the plaintiffs’ claims.
First, the plaintiffs lack standing. To bring a lawsuit in federal court, the plaintiffs must demonstrate that they are personally injured by the FDA’s orders—not merely that they are philosophically opposed to abortion. The plaintiffs cannot make that showing. They are not required to, and in fact do not, prescribe mifepristone to their patients, so they aren’t personally harmed by FDA orders facilitating access to mifepristone.
The plaintiffs’ theory of standing goes like this: (1) Some woman, somewhere in America, might take mifepristone and experience an extremely rare complication; (2) rather than go to her own doctor or a doctor to whom she was referred, she might randomly wander into one of the emergency rooms where the plaintiff-doctors work; (3) there will be no other doctor available in the emergency room, leaving the plaintiff-doctors with no choice but to treat the woman; (4) treating the woman will violate the doctors’ conscience, stress the doctors out, or take them away from something else they’d rather be doing. To guard against this minuscule risk, the plaintiffs want a federal court to ban all women across America from using mifepristone, or at least make it harder for them to get it.

This theory is as wrong as it sounds. Supreme Court precedent establishes that this theory is way too speculative to establish standing.
Second, even if the plaintiffs had standing, their claims fail on the merits. In a nutshell, the plaintiffs argue that the FDA’s orders are “arbitrary and capricious” because the FDA didn’t think hard enough about safety. The plaintiffs are wrong. The FDA did, in fact, think hard enough about safety. The FDA’s decisions were well-reasoned and based on abundant evidence. Under the deferential standard of review, the plaintiffs’ nitpicking of the FDA’s reasoning doesn’t come close to justifying throwing the FDA’s orders out.
The plaintiff-doctors were never personally forced to perform abortions
So how did the plaintiffs’ theories fare during the oral argument?
First, a caveat. I thought the plaintiffs’ attorney was excellent. She answered all questions directly and clearly. Oral argument in the Supreme Court is stressful and challenging, and the attorney did the best job she reasonably could have with a very difficult case. On certain issues, I respectfully disagree with the attorney’s interpretation of the record, but it is not my intention to criticize the attorney’s performance in any way. Instead, the purpose of this post is to assess the strength of the plaintiffs’ arguments, as crystallized at the oral argument.
Let’s start by addressing the plaintiffs’ contentions at the oral argument regarding the individual doctors’ standing. The plaintiff-doctors contend that they face the risk of randomly encountering a woman encountering a mifepristone complication in the emergency room. To support their claims, the plaintiff-doctors submitted declarations to the district court purportedly attesting that they’ve faced these situations in the past; this shows, they claim, that they face the risk of facing these situations in the future.
I seriously doubt that, even if a plaintiff-doctor could attest to having been in such a situation in the past, the plaintiff-doctor would have standing to seek an order banning or restricting all women across America from obtaining mifepristone. But the declarations suffer from an even more fundamental flaw: none of the doctors are able to show any personal harm from the FDA’s actions, even in the past. Most of the declarations speak in general terms about mifepristone being bad. The doctors don’t substantiate that they have a personal stake in the case.
Several Justices press the plaintiffs’ attorney on this issue, including Justice Kagan, leading to the following exchange:
JUSTICE KAGAN: But, if you had to pick one and say go read that declaration and that declaration is going to tell you why -- why, you know, we’re entitled to be up here, who’s the person?
MS. HAWLEY: So I have to pick two, Your Honor, but Dr. Francis and Dr. Skop.
Starting with Dr. Francis, the attorney contends that, in the past, Dr. Francis personally was required to perform an abortion as a result of a patient’s unsuccessful use of mifepristone, giving rise to an inference that the same situation will occur in the future:
JUSTICE KAGAN: Has she ever been -- because I -- I read that declaration pretty carefully. Has -- what actual emergency treatment has she participated in that she objects to and that -- and that she has stated an objection to?
MS. HAWLEY: So the prior page, Your Honor, JA 154, talks about a D&C which she was required to perform due to a life-threatening emergency.
JUSTICE KAGAN: She herself performed that?
MS. HAWLEY: That is correct, Your Honor.
JUSTICE KAGAN: And did she have an opportunity to object? Did she object?
MS. HAWLEY: No, Your Honor. Again, these are life-threatening situations in which the choice for a doctor is either to scrub out and try to find someone else or to treat the woman who’s hemorrhaging on the –
JUSTICE KAGAN: Well, usually –
MS. HAWLEY: -- emergency room table.
Later in the argument, the attorney again takes the position that, on JA 154, Dr. Francis attests that she personally was required to perform a D&C abortion:
JUSTICE KAGAN: But you just said, again, it’s being involved in completing an elective abortion, so I took that to be the conscience objection.
I think what Justice Jackson is asking or what I asked before or what Justice Barrett is, is there any broader conscience objection that appears -- I don’t -- I’m not sure I care all that much about the district court, but that appears in the declarations?
MS. HAWLEY: Yes, Your Honor. And -- and in this sense, completing an elective abortion means removing an embryo, a fetus, whether or not they’re alive, as well as placental tissue. Again, Dr. Francis talks about being required to perform a D&C -- this is at 154 --
JUSTICE KAGAN: So --
MS. HAWLEY: -- and remove placental tissue.
The attorney’s characterization of Dr. Francis’s declaration is, in my view, incorrect. Here is what Dr. Francis’s declaration says on JA 154:
As an additional example, a partner of mine and I cared for another patient who also suffered complications from chemical abortion. I had taken care of her when she was hospitalized for hyperemesis gravidarum at 9 weeks 5 days gestation. She was discharged home in good condition after significant improvement with medications. During that hospital stay, she had an ultrasound, which showed a healthy pregnancy with no apparent complications and a strong fetal heart rate. During her hospitalization, she expressed to me that she was considering abortion because of experiencing hyperemesis but was unsure. Approximately one week after her discharge, the patient presented back at our emergency room with heavy vaginal bleeding and unstable vital signs as a result of taking chemical abortion drugs. One of my partners was able to detect a fetal heartbeat. Due to the amount of bleeding that she was experiencing and evidence of hemodynamic instability, however, my partner had no choice but to perform an emergency D&C. The patient needed to be hospitalized overnight for close observation after the D&C. Not only did my partner need to provide several hours of critical care for this patient, but my partner also needed to call in a back-up physician to care for another critically ill patient. And because the preborn baby still had a heartbeat when the patient presented, my partner felt as though she was forced to participate in something that she did not want to be a part of—completing the abortion.
Dr. Francis does not state that she performed a D&C abortion herself. Instead, Dr. Francis states that she cared for the patient before the patient decided to get an abortion. It was her “partner” who had to perform the emergency abortion. Even setting aside the extreme unreliability of Dr. Francis’s recounting of her anonymous “partner’s” diagnosis and treatment of this anonymous patient, the “partner’s” negative experience doesn’t establish that Dr. Francis was injured, much less that she faces a risk of injury in the future.
One other paragraph of Dr. Francis’ declaration refers to a D&C abortion:
As an example of how chemical abortion harms my patients and my medical practice, one of my patients had obtained mifepristone and misoprostol from a website, without an in-person visit. She was told that the drugs would come from India. After taking the chemical abortion drugs, she began having very heavy bleeding followed by significant abdominal pain and a fever. When I saw her in the emergency room, she had evidence of retained pregnancy tissue along with endometritis, an infection of the uterine lining. She also had acute kidney injury, with elevated creatinine. She required a dilation and curettage (D&C) surgery to finish evacuating her uterus of the remaining pregnancy tissue and hospitalization for intravenous (IV) antibiotics, IV hydration, and a blood transfusion. I spent several hours with her the day of her surgery/hospital admission, keeping me from my primary patient responsibilities in the labor and delivery unit and requiring me to call in an additional physician to help cover those responsibilities.
This paragraph also does not say that Dr. Francis herself performed a D&C. Instead, it recites that the patient “required” a D&C surgery and that Dr. Francis “spent several hours with her the day of her surgery/hospital admission.” Spending several hours with a woman is different from performing an abortion on that woman.
I am also struck by this statement about Dr. Francis:
MS. HAWLEY: So I think, Your Honor, that might be impracticable. If we’re thinking again about the emergency room situation, would Dr. Francis, again, have to know when she’s in the emergency room whether this is a miscarriage, an ectopic pregnancy, or an elective abortion? This is what she does day in and day out.
Dr. Francis’s declaration does not, in my view, support the assertion that she is in these emergency room situations “day in and day out.” I would also note that Dr. Francis is now the CEO of the American Association of Pro-Life Obstetricians and Gynecologists, one of the plaintiff organizations, so I wonder whether she is really seeing patients in the emergency room “day in and day out,” thus entitling her to an order restricting all women across America from obtaining mifepristone.
The plaintiffs’ attorney similarly argues that Dr. Skop was personally required to complete abortions:
JUSTICE JACKSON: It’s -- sorry. It’s my understanding that sometimes the completion, it doesn’t involve surgical intervention. Do you have a sense of how often? I mean, we -- we may get all the way down the chain to the doctor’s there, the person is having an emergency procedure. My understanding is, with some of these chemical abortion scenarios, the completion occurs by prescribing additional medication. Do you have a sense of how many times the completion is that route and could be done by another physician as opposed to your clients doing a -- a medical procedure?
MS. HAWLEY: So -- so that second dose, Your Honor, of misoprostol has been part of the regimen since 2016, really I think all the way back to 2001, but -- but it’s been approved by FDA since 2016. So the best numbers we have from FDA are still consistent with that, and that means that 3.1 percent of pregnancies at 10 weeks will be ongoing. I -- I’d encourage you to look at -- at JA 405 through 407, and this explains that these risks go up without an in-person visit.
JUSTICE JACKSON: Yeah, no, I guess I’m just trying to get at -- we’re still -- I’m still working on how many circumstances or how often it would be that your clients actually have to complete the procedure in the way that you are describing.
MS. HAWLEY: So Dr. Skop talks about doing this at least a dozen times, either a D&C or a suction-aspiration abortion to remove, again, embryos, fetuses, or placental tissue.
In context, Justice Jackson is asking the attorney how often her clients have to complete an abortion as opposed to a different doctor completing the abortion. The attorney’s response that “Dr. Skop talks about doing this at least a dozen times” suggests that Dr. Skop had to complete an abortion at least a dozen times.
Dr. Skop’s declaration does not say this. Instead, it says:
In my practice, I have cared for at least a dozen women who have required surgery to remove retained pregnancy tissue after a chemical abortion. Sometimes this includes the embryo or fetus, and sometimes it is placental tissue that has not been completely expelled.
This paragraph does not represent that Dr. Skop ever had to complete an abortion. Instead, it says that she “cared” for women “who have required surgery to remove retained pregnancy tissue after a chemical abortion.” In other words, some other doctor performed the surgery and she “cared” for that patient.
Also, Dr. Skop does not state in her declaration that this poses a conscience violation. Nor does she claim to have been harmed by “caring” for those patients in any other respect. Instead, this statement appears in a portion of the declaration explaining that “[t]he drugs mifepristone and misoprostol may cause serious complications for the women and girls who take them.” In other words, she’s explaining how the drugs harm other people, not her.
Dr. Skop does later represent in her declaration that “[t]he FDA’s expansion of chemical abortion also harms my conscience rights because it could force me to have to surgically finish an incomplete elective chemical abortion.” But notice the conditional term there: “could.” Dr. Skop is careful not to state in her declaration that she ever had to “surgically finish an incomplete elective chemical abortion” a single time in her entire life.
Justice Barrett recognizes this deficiency in the declarations, leading to the following back-and-forth:
JUSTICE BARRETT: Ms. Hawley, can I take you back to the affidavits and some of Justice Kagan’s questions? You were talking about Dr. Francis. And as I read her allegations or her -- as her affidavit reads, she said that her partner was forced to perform a D&C when there was a living fetus, and she said she performed a D&C on a woman who was suffering serious complications, but the fact that she performed a D&C does not necessarily mean that there was a living embryo or a fetus because you can have a D&C after, you know, a miscarriage. So, if that’s right, I mean, I think the difficulty here is that at least to me, these affidavits do read more like the conscience objection is strictly to actually participating in the abortion to end the life of the embryo or fetus, and I don’t read either Skop or Francis to say that they ever participated in that. So do you want to address that?
MS. HAWLEY: Sure. So, first, Justice Barrett, I think Dr. Francis’s, combined with CMDA, can be read for the broader conscience harm. Again, that’s how the district court understood that. I’d point you to pages 7 and 8. That’s how both the state panel and the Fifth Circuit understood Respondents’ conscience harms to extend beyond simply requiring the ending of an unborn life. And with respect to even the more narrow conscience harm, to whether a doctor may need to end a life, we think there’s still a substantial risk of that occurring. If you look at the numbers of the increase from 7 to 10 weeks in gestational age, that means that 3.1 percent of pregnancies will be ongoing, requiring a D&C. We know at JA -- or, excuse me, ROA 870, that 55 percent of those D&Cs occur in the emergency room.
The bolded statement is intended to substantiate the plaintiffs-doctors’ theory that they face a substantial risk of encountering a woman in the ER who previously took mifepristone and now needs a surgical abortion.
The attorney offers no record citation for the proposition that “3.1 percent of pregnancies will be ongoing, requiring a D&C,” and I did not see that statement in the brief, but I will assume that it is accurate. Even so, that number is relevant only if those women receive their D&C abortion in the emergency room—and hence might theoretically encounter the plaintiff-doctors. If the abortion is performed as part of a scheduled procedure, it cannot possibly affect the plaintiff-doctors, who don’t participate in scheduled abortions. That’s why that “55 percent” figure is crucial.
I have followed this litigation very closely, and I have never seen that 55 percent figure before. So I took a look at ROA 870. This page appears in a study in which one of the plaintiff-doctors (Dr. Harrison) is a co-author. Dr. Harrison attests that she wrote it as part of her “duties and responsibilities” at the now-former CEO of the American Association of Pro-Life Obstetricians and Gynecologists. ROA 870 is pasted below:

Your guess is as good as mine as to where the “55%” figure came from.
To wrap up this discussion, I find it pretty amazing that the plaintiffs’ declarations are unable to identify a single solid example of any of the plaintiffs being harmed by mifepristone in the past. These plaintiffs were hand-picked for this suit. Their co-plaintiff is an organization created for the specific purpose of bringing this suit. Their declarations were no doubt reviewed by highly sophisticated attorneys. The declarants have never been cross-examined or deposed, so the declarations reflect the best possible versions of their arguments. And yet, still, not a single plaintiff is able to substantiate any past harm. This might be the single strongest piece of evidence that mifepristone is safe.
Banning mifepristone will not help the plaintiff-doctors study it.
The plaintiff-organizations also claim to have organizational standing—that is, they claim that they suffered an injury independent of the injury suffered by the physicians. Here’s the basic theory, as expressed during the oral argument:
If you look at how our organizations have been harmed, they’ve been forced to divert resources from speaking and advocating for their pro-life mission generally to explaining the dangers of the harm from abortion drugs.
This argument, if accepted, would obliterate all limitations on Article III standing. Literally any time any federal agency does anything that an organization thinks is bad, the organization could claim that it has been forced to divert resources so as to explain why that thing is bad. This means that any time any organization disagrees with anything the government does, it can sue.
This isn’t the law. The plaintiffs attempt to ground their argument in a case called Havens Realty v. Coleman, but Havens Realty doesn’t stand for that proposition. In Havens Realty, the organizational plaintiff’s mission was to “assist equal access to housing through counseling and other referral services.” The organization was challenging the defendants’ practice of “racial steering”—that is, lying to racial minorities about the availability of housing so as to steer them to live somewhere else.
It’s easy to see why the organization had standing. The organization was devoted to helping racial minorities find places to live; the defendants falsely claimed housing was unavailable, thus hindering the organization from finding those places to live. As the Court put it, “[s]uch concrete and demonstrable injury to the organization’s activities — with the consequent drain on the organization's resources — constitutes far more than simply a setback to the organization’s abstract social interests.” This decision does not suggest that an organization can challenge any rule it disagrees with, as the plaintiffs in FDA v. AHM claim.
In an effort to fit the plaintiffs’ claim within the Havens Realty framework, the attorney points to the FDA’s decision in 2016 that it was no longer necessary to collect certain information about mifepristone’s adverse effects. When mifepristone was approved in 2000, the FDA required prescribers to report all serious adverse events—both fatal and non-fatal. In 2016, at the same time that the FDA made changes to mifepristone’s conditions of use, the FDA decided that, going forward, prescribers would only have to report fatal events. According to the plaintiffs’ attorney, that aspect of the FDA’s order harmed the plaintiff organizations’ mission of studying the adverse effects of mifepristone:
For example, if the regulations are put back in place, the protections whereby individual abortion providers need to provide information about adverse events, that would provide our Respondent organizations with more accurate information about the harms from abortion drugs.
The attorney later makes the same point in an exchange with Justice Barrett:
JUSTICE BARRETT: Explain to me what additional costs you might have incurred or how your resources were diverted in a way that would satisfy Havens.
MS. HAWLEY: Absolutely, Your Honor. So putting to the one side the citizen petition, the AAPLOG declaration is clear that Respondent organizations conducted studies and analyzed studies. This included going through the Medicaid data. It included going through the FAERS data to the extent it was available.
JUSTICE BARRETT: Is that it?
MS. HAWLEY: Well -- well, those studies, Your Honor, I would point to you, one of them is at ROA 5 -- excuse me -- ROA 870 and before and after. And those are pretty comprehensive studies, Your Honor.
JUSTICE BARRETT: And are they to the end of the litigation and the citizen petition, or what are they to the end of?
MS. HAWLEY: To accurately assess the harm from abortion drugs, Your Honor. So I think it’s absolutely separate from the litigation.
(ROA 870 is the page from the joint appendix that’s pasted above that doesn’t support the “55 percent” statistic).
Well, OK, I accept the premise that if an organization’s mission is to analyze data, then it has standing to challenge an agency order that prevents it from obtaining that data. But the plaintiffs aren’t asking for more data to be collected. They’re asking for a court order that would ban or restrict all women from obtaining mifepristone! As a general rule, banning or restricting access to a thing decreases, rather than increases, data about that thing.
It’s true that the FDA stopped mandating prescriber reports in 2016, so there’s going to be less information about the effects of the 2016 and 2021 changes than if the FDA didn’t do that. But the plaintiffs aren’t asking to reinstate a reporting requirement to assess the effect of any post-2016 changes. Instead, they’re asking the court to roll back the 2016 and 2021 changes to mifepristone’s conditions of use, thus making it impossible for any data to be collected regarding these changes. I look forward to a lawsuit in which a plaintiff argues that all gas stoves should be banned so it can obtain more data on whether gas stoves are safe.
I can’t help but note the extreme weakness of the plaintiffs’ challenge to the FDA’s decision regarding the reporting requirement. There’s no statute that requires the FDA to impose this reporting requirement. The reporting requirement doesn’t exist for most drugs. It’s entirely within the FDA’s discretion.
In 2016, the approving official concluded: “After 15 years of reporting serious adverse events, the safety profile of Mifeprex is essentially unchanged. Therefore, I agree that reporting of labeled serious adverse events other than deaths can be collected in the periodic safety update reports and annual reports to the Agency.” In 2021, the FDA rejected a challenge to this change to the reporting requirement, explaining its decision as follows:
We acknowledge that there is always a possibility with any drug that some adverse events are not being reported, because reporting to the Agency’s MedWatch program by health care professionals and patients is voluntary. We do not agree, however, that the 2016 changes to the prescriber reporting requirements limit our ability to adequately monitor the safety of mifepristone for medical termination of pregnancy. Prior to the 2016 approval of the S-20 efficacy supplement, we assessed approximately 15 years of adverse event reports both from the Applicant and through the MedWatch program and determined that certain ongoing additional reporting requirements under the Mifeprex REMS, such as hospitalization and blood transfusions, were not warranted. This assessment was based on the well-characterized safety profile of Mifeprex, with known risks occurring rarely, along with the essentially unchanged safety profile of Mifeprex during this 15-year period of surveillance. Accordingly the Prescriber Agreement Form was amended as part of our 2016 approval of the S-290 efficacy supplement to require, with respect to adverse event reporting, only that prescribers report any cases of death to the Applicant.
The FDA also pointed out that the drug manufacturer does have to report non-fatal serious adverse events:
We also note that the reporting changes to the Prescriber Agreement Form as part of our 2016 approval do not change the adverse event reporting requirements for the Applicants. Like all other holders of approved NDAs and ANDAs, the Applicants are required to report all adverse events, including serious adverse events, to FDA in accordance with the requirements set forth in FDA’s regulations. FDA also routinely reviews the safety information provided by the Applicants in the Annual Reports. As with all drugs, FDA continues to closely monitor the postmarketing safety data on mifepristone for the medical termination of pregnancy.
To me this reasoning seems completely rational. It doesn’t violate any statute. I don’t understand how a court could possibly say this is arbitrary and capricious.
The FDA knows how to evaluate studies
Let’s turn to the merits. The plaintiffs seek to overturn both the 2016 and 2021 changes to mifepristone’s conditions of use.
As noted above, in 2016, the FDA increased the gestational age limit from 49 to 70 days, reduced the number of required in-person clinic visits to one, and allowed healthcare providers other than doctors to prescribe the drug. With regard to those changes, the plaintiffs’ basic point, as expressed at the oral argument, is that the FDA “failed to consider or explain the cumulative effects of its wholesale removal of safeguards.” The attorney says this:
In 2016, what the FDA said was we’re going to look at individual studies and then, even though we say they’re interrelated at JA 298, we’re going to take all of the protections away at once.
The attorney’s implication is that the FDA looked at only “individual studies”—i.e., studies that addressed individual changes—despite its acknowledgment that the changes are “interrelated.” Did the FDA really say that?
No, it did not. Here’s the discussion from JA 298 in which the word “interrelated” appears:
The clinical review team identified several major proposed clinical changes in the efficacy supplement. As these major changes are interrelated, in some cases data from a given study were relied on to provide evidence to support multiple changes.
The FDA is saying the exact opposite thing: because the changes are “interrelated,” it is analyzing studies that report the effects of multiple changes. So no, the FDA didn’t “fail[] to consider or explain the cumulative effects of its wholesale removal of safeguards,” as the attorney represents.
As for the FDA’s 2021 decision to eliminate the in-person dispensing requirement, the opening stanza of the attorney’s argument is: “FDA approved abortion by mail based on data it admitted was ‘not adequate.’” Did the FDA—the most neurotic organization on Earth—really approve a change “based on” admittedly inadequate data?
No, it did not. Later in the argument, the attorney cites “JA 407” for this proposition, so let’s take a look at what the FDA says on JA 407:
While the studies we reviewed are not adequate on their own to establish the safety of the model of dispensing mifepristone by mail, the safety and efficacy outcomes reported in these studies remain within the ranges labeled for the approved mifepristone products. Although the literature suggests there may be more frequent ED/urgent care visits related to the use of mifepristone when dispensed by mail from the clinic, there are no apparent increases in other significant adverse events related to mifepristone use.
Based on the REMS assessment data, FAERS data from the time period when the in-person dispensing requirement was not being enforced, and our review of the literature, we conclude that mifepristone will remain safe and effective if the in-person dispensing requirement is removed.
As the full discussion makes clear, the FDA did not approve a change “based on data it admitted was ‘not adequate.’” Instead, the FDA said that certain studies it reviewed “are not adequate on their own.” But the FDA then explained that those studies, when viewed in conjunction with two other sources of data, formed a sufficient basis to make the change. Saying “we’re approving a change based on data that are not adequate” is completely different from saying “these studies aren’t adequate on their own, but all of the data put together are, collectively, adequate.”
The plaintiffs also quibble with particular studies in the agency record. For example, consider this exchange:
JUSTICE BARRETT: So General Prelogar said that that initial in-person visit had no requirement of an ultrasound or, you know, any effort to detect fetal heartbeat, so it wouldn’t necessarily give an accurate read on gestational age or detect an ectopic pregnancy. So why would that necessarily -- the elimination -- why would the elimination of the visit necessarily increase the risks?
MS. HAWLEY: So I think, Your Honor, FDA’s own data shows that those risks did go up. If you look at the Kerestes study, it shows a nearly threefold increase in emergency room visits when you have the in-person visit and when you removed it. There was 5.8 percent with an in-person visit, and it was also -- and about 2.1 without.
Here’s the relevant excerpt from the record:
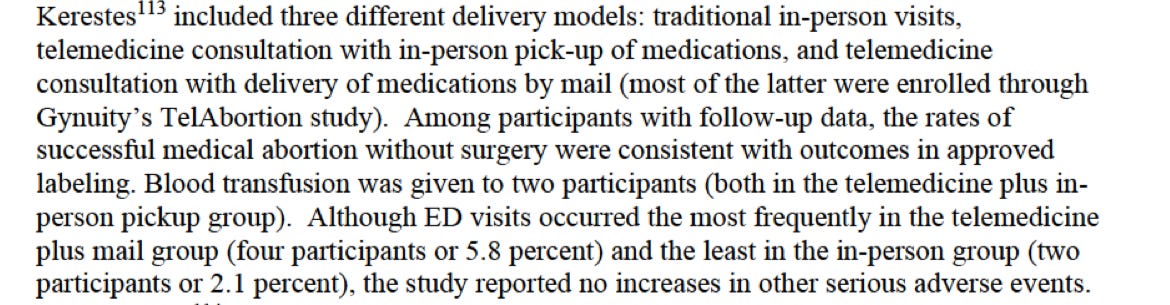
The Kerestes study shows that four participants from one group visited the ER, and two participants from another group visited the ER, but there were no differences in “other serious adverse events.” This study was one of the studies that led the FDA to conclude that the studies are “not adequate on their own” to reach a firm conclusion. This seems like a rational conclusion—indeed, given the extremely underpowered nature of this study, it seems like the only rational conclusion on this record. If the FDA were to claim that this four-versus-two distinction supported the inference that eliminating the in-person dispensing requirement would yield a “nearly threefold increase in emergency room visits,” that would be arbitrary and capricious, at least in my opinion.
***
Takeaway from oral argument: I continue to be unpersuaded by the plaintiffs’ arguments.
My guess is that the Supreme Court will rule that the plaintiffs lack standing and won’t reach the merits. We’ll find out soon.
We are again indebted to the author for a painstaking look at the record, powerful analysis, and clear exposition of a case I would otherwise understood only superficially. His reticence about explicitly criticizing Sen Hawley's wife is forgivable since as Marty’s comment shows a reader can easily see her unprofessional dishonesty in a case she volunteered to argue.
Thanks for the detailed discussion of the evidence, or lack of it, provided by the plaintiffs here. I've seen innumerable articles dissecting the standing arguments but few get as far as you in looking at the merits